During the 18 months since Addenbrooke’s Hospital installed a solution that uses active radio frequency identification tags to track medical equipment, the 1,100-bed medical facility reports that it has more than doubled its asset-utilization rate, thereby reducing the need for excess rentals and purchases, as well as the amount of time employees previously spent searching for missing items. By the end of this year, the hospital expects a total of approximately 10,000 pieces of equipment to have been fitted with active tags. In addition, the facility is piloting the use of ultrahigh-frequency (UHF) passive tags for some of its other lower-value or less-mobile goods.
The British research hospital installed the technology, provided by RFID systems integrator Harland Simon, to monitor medical assets loaned from its Medical Equipment Library (MEL). Addenbrooke’s also uses the technology to track other mobile items, including all 1,000 of its beds, wheelchairs and mobile pumps destined for surgical units.

Addenbrooke’s is part of the Cambridge University Hospitals National Health Service (NHS) trust, and one of the nation’s largest and most renowned medical facilities. The challenge for Addenbrooke’s, as with many hospitals, is locating assets when they are needed. Its Medical Equipment Library is responsible for thousands of items (every month, it loans nearly 2,000 pieces of equipment to about 45 specific departments) that must then be retrieved by MEL’s staff for reuse elsewhere.

Problems arise when the equipment can no longer be located at the department that had borrowed it. Frequently, a particular asset may follow a patient who has been moved to another department, for example, and finding that item can thus prove very time-consuming. Such items often become “long-term loans,” meaning they are not returned for reuse and may or may not even be in use at the time.
Prior to the RFID system’s installation, MEL’s staff would regularly conduct departments audits to locate missing equipment, walking through each department and recording anything they might find. This process could take about two days to complete. The facility thus considered several other solutions, including a Wi-Fi-based real-time locating system (RTLS), but found many to be unrealistic due to the cost of installing the infrastructure, says Simon Dawkins, the Medical Equipment Library’s supervisor. The hospital currently does not have a Wi-Fi network installed.
Harland Simon, which has provided RFID-based asset-management technology for several years, supplied a relatively inexpensive and easy-to-install RFID solution that could be integrated with Addenbrooke’s existing equipment-management software. The solution employs RFID tags and readers manufactured by Taiwanese company Syris, using Harland Simon’s proprietary design. Addenbrooke’s deployment consists of active 2.4 GHz tags affixed to assets, 13 fixed readers with a 40-meter (131-foot) read range installed at key chokepoints, and a half-dozen handheld reading devices for collecting location data within areas where tags are out of range of the fixed interrogators. Data culled from the readers is managed by Harland Simon’s RFID Discovery software, which tracks each item’s “last seen” read event and shares that information with the equipment-management software.
First, a Harland Simon 2.45 GHz active tag is attached to each asset, and is entered into the hospital’s system by means of a handheld reader, with a worker inputting asset data along with the tag’s unique ID number. A fixed reader in the MEL area interrogates the tag, which beacons approximately every 20 seconds. When an employee borrows an infusion pump, feeding device or other asset, a MEL worker enters data in the equipment-management software, thereby indicating which ward is borrowing that item.
Once the equipment is removed from the library, the reader ceases to detect its tag and updates that item’s status in the RFID Discovery software, which then forwards the information to MEL’s management software. At some locations throughout the facility, the tag passes a fixed reader, which transmits the read data back to the RFID software via a cabled connection, indicating the asset’s latest “last seen” location. That data is then fed into MEL’s management software as well.
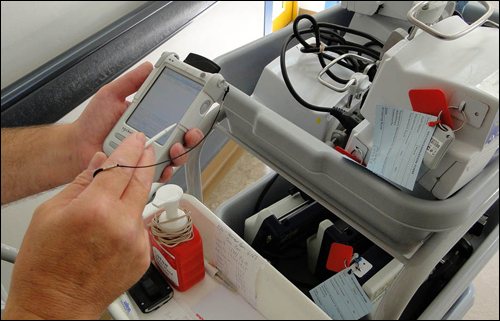
When visiting a ward to pick up or drop off a particular piece of equipment, MEL’s personnel carry a PDA equipped with a built-in reader. As a worker enters a ward, he or she selects that area via a drop-down menu in the handheld’s software, and then selects a prompt to launch an audit. The reader interrogates all tags within about 20 meters (66 feet), listing not only all assets within that ward, but also any that may have an imminent maintenance requirement.
Before the system was taken live, the hospital loaned infusion pumps on an average of 1,000 to 1,200 times per month. Now, that number has increased to more than 3,000. The loan rate of other devices, such as syringe drivers—small infusion pumps used to deliver IV medications—feeding devices and monitors have also increased, though less dramatically. In January 2011, MEL identified the delivery of 1,526 devices to various departments. By March of this year, the quantity of loaned equipment had more than doubled, according to the facility. What’s more, the amount of time that equipment spends in active use has risen from 5 percent to about 40 percent. Given the increased loan and utilization rates for each asset, the hospital has been able to reduce its need to rent or purchase equipment, and has thus saved around $200,000.
In addition, with the RFID-based solution in place, equipment inventory audits that once required two days of labor now take just 30 minutes to complete. The number of long-term loans has dropped as well, by about 35 percent.
According to Dawkins, the technology can also be used to monitor the performance of contractors cleaning or maintaining equipment. The hospital has installed a fixed reader at the egress to a cleaning area for beds, where a third-party contractor sanitizes each bed before it can be returned to a patient room. The process should take about seven minutes, he notes, but the technology revealed that in some cases, tagged beds passed through the procedure in only a minute or two, potentially indicating that it was not being properly cleaned.

Addenbrooke’s was able to work with the contractor to ensure that the problem was resolved, Dawkins reports. The software also allows the hospital to identify when beds become backed up while awaiting sanitization, or to be returned to patient rooms. “In fact,” he states, “we discovered we had too many beds.” Therefore, as the facility has expanded some of its patient services, it has not needed to purchase additional beds to accommodate that growth, since it already had surplus beds on hand.
To date, Addenbrooke’s Hospital has attached active tags to about 4,000 pieces of equipment and mobile devices. This week, the facility began testing the use of passive UHF RFID tags to track lower-value assets. Initially, equipment in the radiology department is being tracked via the UHF system, which consists of a combination of tags made with Alien Technology and Impinj RFID chips and an Alien handheld reader, using the same RFID Discovery software.
Radiology vests, as well as imaging machinery and other large equipment, are currently being tagged, Dawkins says, and the hospital is testing read ranges with a variety of tags affixed at different locations. This testing will continue for about three months, he explains, after which Addenbrooke’s will determine whether (and how) to deploy passive technology as part of its RFID solution. “We didn’t just buy a system,” he states, adding, “We’re growing the system. We have a continued working relationship” with Harland Simon.